


For doctors:
- When choosing an anticoagulant for AF, it speeds up the decision-making process at times. This speed is achieved by using complex variables and all related parameters of all scales and formulas (Cockcroft-Gault, CKD-EPI, HAS-BLED, CHA2DS-VASC with the latest corrections) are entered once, not several times for each calculation! Parallel accounting for the presence / absence of ACS. Accounting for the presence/absence of stents in the coronary bed. That allows you to get the best recommendation. The calculation takes place on the fly, each new parameter instantly corrects the result (you can observe the intermediate one), but the most important thing is that you do not stay with the calculation results, but immediately receive a recommendation in text form, verified with the latest recommendations. You dont even need internet for this.
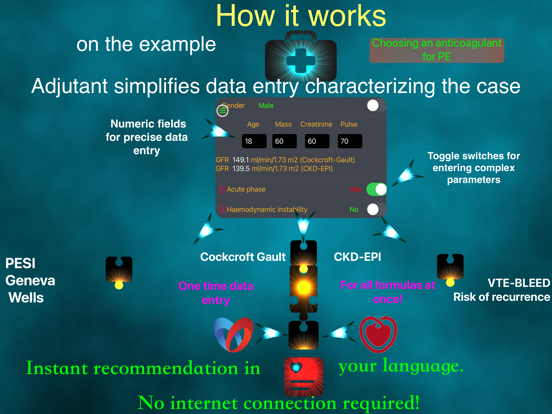
- When choosing an anticoagulant for PE/DVT, using the techniques described above, the program simultaneously calculates all the necessary scales and formulas (Geneva, Wells, PESI, Cockcroft-Gault, CKD-EPI, thrombosis recurrence predictive scale, VTE-BLEED, etc.).
- Algorithm for the use of rivaroxaban 2.5 mg.
- Collective scale of modification of the risk of bleeding (significant and non-significant). The scale is a composite of HAS-BLED, HEMORR2HAGES, ABC. You wont see this anywhere else.
- Collection of articles on AF and anticoagulant therapy (Internet connection required)
- Links to various educational events that deal in one way or another with the topic of anticoagulant therapy or the treatment of AF (internet connection required).
For teachers, lecturers, students:
- Allows you to easily and quickly simulate patients of varying complexity
- Using the application, you can quickly create clinical tasks (thematic)
- Can be helpful in mastering the recommendations
For patients:
- Simplified calculators for self-control.
- Self-learning information on atrial fibrillation, with different feed levels.
Disclaimer.
- the author does not bear any responsibility for the consequences that followed the use of the recommendations that the program generates.
- recommendations are advisory in nature and are not a guide to action.
- if you are not a certified medical specialist, then always remember that you should never use the recommendations generated by the program without consulting your doctor!
- if you are a specialist in the field of medicine, then all the responsibility for making a decision in a specific clinical situation lies with you (as always). Program recommendations are only supportive. Only you decide whether to use the information received or not.
Links:
- RSC recommendations from 2020 AF (https://scardio.ru/content/Guidelines/2020/Clinic_rekom_FP_TP.pdf)
CAD (https://scardio.ru/content/Guidelines/2020/Clinic_rekom_IBS.pdf)
- EHRA recommendations from 2021
AF (https://academic.oup.com/europace/article/23/10/1612/6247378#237648358)
- ESC recommendations from 2020:
AF (https://www.escardio.org/Guidelines/Clinical-Practice-Guidelines/Atrial-Fibrillation-Management)
ACS (https://www.escardio.org/Guidelines/Clinical-Practice-Guidelines/Acute-Coronary-Syndromes-ACS-in-patients-presenting-without-persistent-ST-segm)
- ESC with ERS Guidelines 2019:
PE(https://academic.oup.com/eurheartj/article/41/4/543/5556136)
- ESC consensus document 2017:
DVT(https://academic.oup.com/eurheartj/article/39/47/4208/3002647)
- CKD-EPI (https://pubmed.ncbi.nlm.nih.gov/19414839/)
- SCF Cockcroft-Gault (https://pubmed.ncbi.nlm.nih.gov/1244564/)
- Geneva (revised) (https://pubmed.ncbi.nlm.nih.gov/16461960/)
- HEMORR2HAGES (https://pubmed.ncbi.nlm.nih.gov/16504638/)
- ABC (https://academic.oup.com/eurheartj/article/37/20/1582/2570476)
- Wells rule (https://pubmed.ncbi.nlm.nih.gov/11453709/)
- PESI (https://pubmed.ncbi.nlm.nih.gov/16020800/)